
ECG of the Week 1 February 2023 – Interpretation
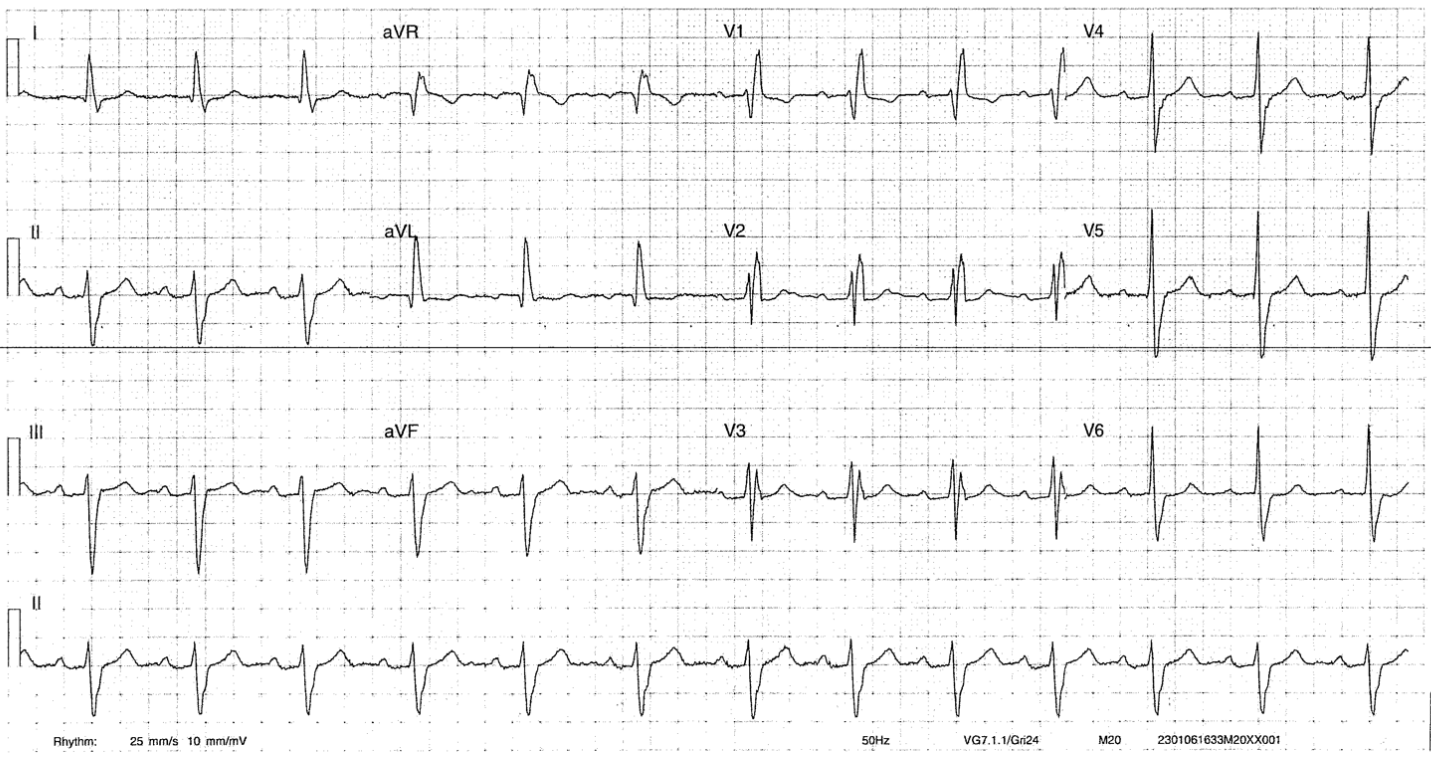
The patient is in sinus rhythm with a rate of approximately 75. There is PR prolongation signifying first degree AV nodal block at 210ms or so. The QRS axis is a left axis deviation. Additionally, the QRS complex is wide with a right bundle branch block pattern. In the context of RBBB, the left axis deviation signifies a left anterior fascicular block too. In summary, the patient has a first degree AV block and bifascicular block. Without a clear history of syncope or pre-syncope, there isn’t an absolute indication for pacemaker placement. It is possible that the palpitations experienced may be episodes whereby conduction through the remaining left posterior fascicle is intermittently blocked and ventricular or junctional escape occurs, but this is postulation.
His troponin were elevated without dynamic increase at approximately 80ng/ml. He was subsequently discharged to have follow up with his cardiologist.
It is also worth noting that valvular surgery (mitral valve surgery more than aortic valve surgery) can lead to nodal blockades due to the proximity of the AV node to the operation site during valve surgery. The risk of AV nodal blockade is highest in the immediate post-operative period and most surgeons will place epicardial pacing wires post valvular surgery.