
You are reviewing the ECG of a man who has had an intermittent history of chest pain during exercise. His PMH includes being an active smoker but he has no other cardiac risk factors. He is currently pain free. There is a family history of cardiomyopathy.
Observations are P78 BP182/105, T36.8, RR16, Sats 100% on air. ECG as below.
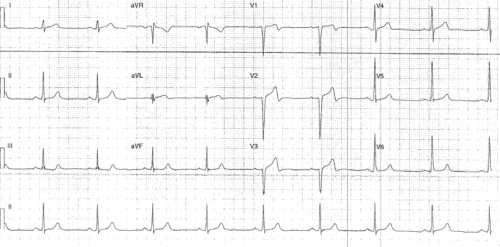
Interpretation:
- Rate: 54
- Rhythm: Sinus rhythm
- Axis: Normal 0-90
- Morphology: Biphasic (+-) TW in V1-3 and aVL, 1mm STD III
- Intervals: PR160 QRS 90 QTc 420
- Summary: Wellens Type A
Disposition:
Wellens syndrome is a combination of the ECG changes seen above with recent and resolved chest pain. It is specific for critical stenosis of LAD and therefore admission for angiogram is imperative (risk of MI in coming days and risk of ischaemia or dysrthymia on stress testing)
Interestingly if ECG is done on these patient whilst in pain there may be ‘pseudo-normalisation’ of T waves
Clinical Closure:
- Trop 108
- Admitted under Cardiology
- Angiogram 80% stenosis proximal LAD (stented) 70% stenosis proximal RCA
Further Reading: Online – for further info on understanding T waves and the different changes seen in Wellens.