
A 32 year old man has presented after developing left sided chest pain whilst shoveling in the garden. He feels sweaty and dizzy. He is a FIFO worker with no medical history.
His observations are: HR 110, BP 160/110, RR 24, Sats 95% air, T36.4
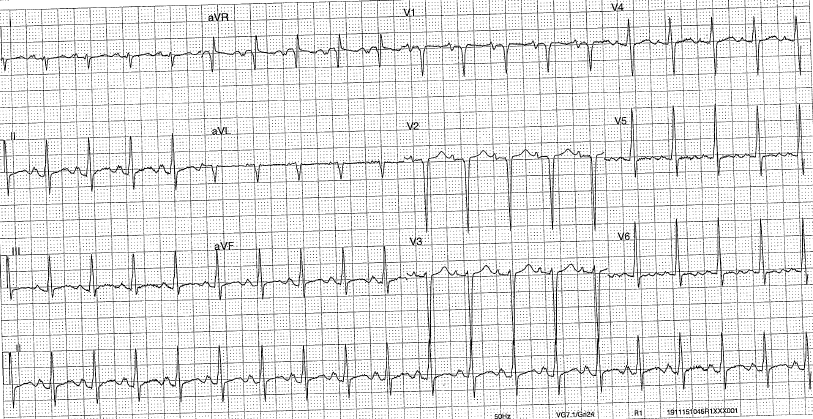
His EGC is as below:
Interpretation:
- Rate: 120
- Rhythm: sinus rhythm
- Axis: RAD +120
- Morphology:
- P waves – biphasic
- QRS – delta pattern, septal Q waves,
- T waves – biphasic, notable in V5-6
- Intervals: QTc 450
Differential Diagnosis:
- Acute coronary syndrome (including vasospastic given age)
- PE
- Aortic Dissection
- Myocarditis
- Cardiomyopathy
Clinical Closure:
- Admitted to regular meth use
- Trop 350 –> 3450
- CXR: prominence of bronchovascular markings and subtle airspace shadowing constant with early signs of fluid overload
- CTPA: no PE or Aortic dissection – again features of APO
- Echo: Diffuse hypokinesis of LV, EF 22%, Moderately dilated RA
- Coronary angio: no abnormalities
- Treated as non ischaemic (METH induced) cardiomyopathy, admitted under cardiologists for 3 days.
- Related to ECG
- Dilated RA = p pulmonale (LAA)
- Poorly functioning LV = RAD, Pseudo WPW likely related to evolving BBB, Q waves in antr leads
- Meth use (other cause not identified) prolonged QTc