
The ECG below is taken from a collapsed 70kg 56 yo man with a known mental health history, thought to have taken a multi-drug overdose.
On further collateral history it is apparent he has taken the following medications approx. 5 hours prior: Chlorpromazine 975mg, Aspirin 1.4g, Dothiepin 7g and Diazepam 250mg.
On presentation his observations are as follows:
GCS 3
HR 96
BP 100/58
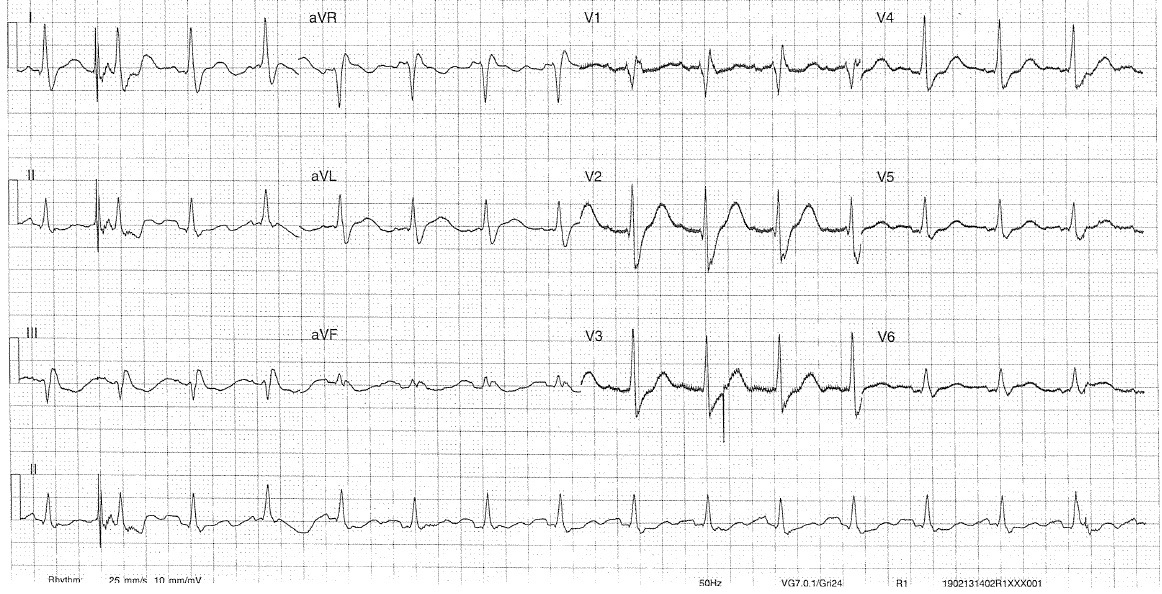
Key Features:
Rate: 90
Rhythm: Sinus
Axis: Normal
Intervals:
- PR 100
- QRS 160 – prolonged – risk of Ventricular Dysrthymia
- QTc 480 – prolonged
Additional:
- Terminal R wave in aVR (R/S ratio >0.7)
Management:
Use an RRSIDEAD toxicology approach:
Resus:
- A: Intubate if GCS <12
- Importance of pre-optimising prior intubation: risk of acidosis during intubation will worsen TCA toxicity.
- B: Hyperventilate (aiming for a pH of >7.5)
- C: Correct hypotension – fluids, NaHCO3, Ad/NAd
- C: Treat Dysrthymias – NaHCO3 2mmol/Kg IV every 1-2mins (aiming for a QRS <100), Lignocaine as 2nd line 1.5mg/Kg when pH>.5, DCCV unlikely to work
- D: Seizures – benzos, bentos, benzos (other antieplieptics ineffective), don’t forget also likely to need NaHCO3 if seizing, consider GA if no cessation (most experienced operator, risk of cardiac dysthymia/arrest on intubation.
Risk:
- 100ml/Kg of TCA Dothiepin = serious life threat
- Those with dosing >30mg/Kg are significant of severe toxicity, symptoms expected within 2 hrs but may last for >24 hrs.
- Severe toxicity overdoses demonstrate pH dependent cardiotoxicity.
- QRS intervals: >100 risk of seizure >160 risk of ventricular dysrthymia
- Aspirin = 20mg/Kg = no to low risk
Supportive Care
Investigations:
- BSL
- ECG
- Paracetamol and Salicylate levels
- VBG
Decontamination
- Activated charcoal indicated in toxicity once airway secure
Enhanced Elimination
- Not indicated in this case
Antidote
- Consider NaHCO3 as an antidote. Give as boluses 1-2mmol/Kg to see effect in QRS
- Together with hyperventilation aim for pH >7.5
Disposition:
- Intubation, ICU
Key Points and Take Homes:
TCA Overdose
- Mechanism of toxicity via Na channel blockade, alpha adrenergic blockade and anticholinergic effect.
- All TCA overdose patients should be cardiac monitored for 6 hrs regardless of symptoms
- >10mg/Kg = potential life threat
- 5-10mg/kg = Mild anticholinergic features and drowsiness
- >10mg/kg = Anticholinergic features may be masked by reduced GCS, Cardiac dysrhythmias, hypotension, risk of seizures,
- >30mg/kg = Severe toxicity. Cardiotoxicity is pH dependent
- ECG intervals: Risk of dysrhythmia with QRS of >160 , Risk of seizure QRS >100
Aspirin Overdose
- >150mg/Kg = acutely toxic dose
- <300mg/kg = moderate toxicity
- 300-500mg/Kg = severe toxicity
- >500mg/Kg = potentially lethal dose
References / Further Reading
Textbook
- Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.