
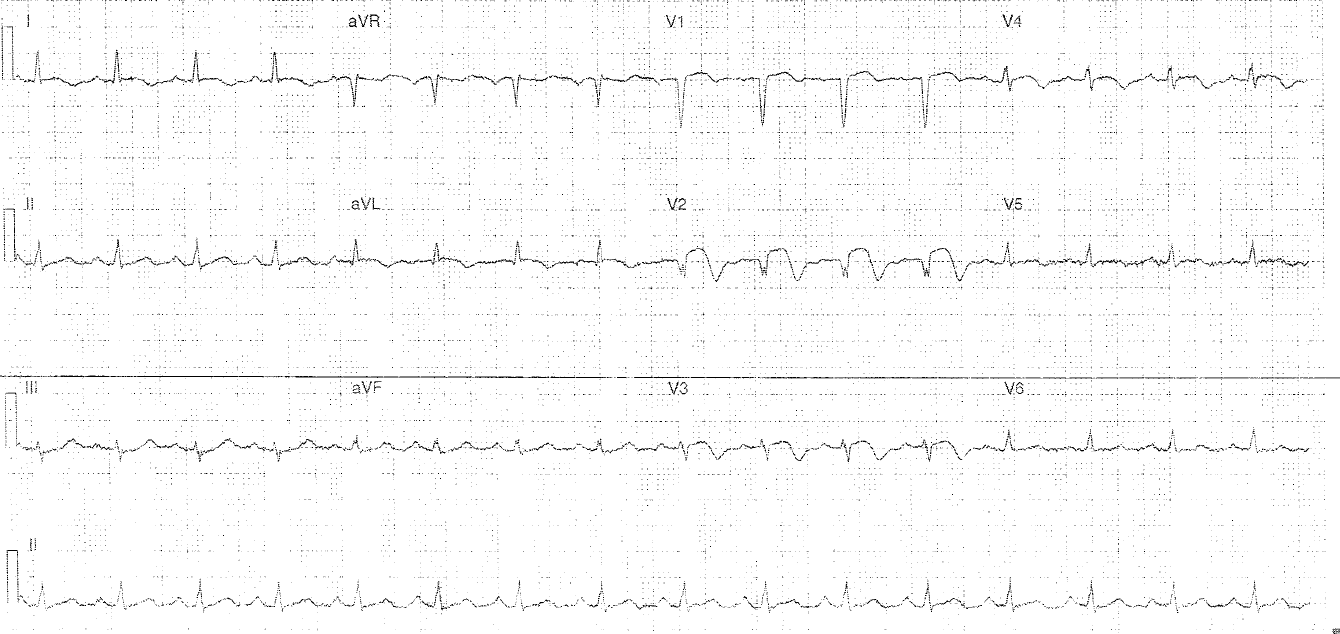
The following ECG is from a patient that has presented with left arm pain:
Interpretation:
- Rate: 96
- Rhythm: NSR
- Axis: Normal
- Morphology: Most obvious abnormality is STE in least V1 to V4 with associated pathological looking T wave inversion. Prominent p waves QRS fragmentation in II, III, aVF, V2, V4
- Intervals: PR 180 QRS 80 QTc 450
- Summary: Consistent with anterior STEMI
- Does this meet Code STEMI criteria for cath lab activation? In Joondalup hospital no – you need 2mm STE in congruent leads other than an inferior distribution (requiring only 1mm STE) – in this instance the case should be urgently discussed with a cardiology consultant on call regarding PCI providing there are no contraindications.
- Interesting discussion – if this had been a 20 year old presenting with syncope would it change your management? These changes could also be considered consistent with saddleback ST change seen with Brugada Type 3 (sodium channelopathy causing patient to be at increased risk of dysrhythmia and sudden cardiac death)
In terms of anatomical occlusion this diagram below is super helpful (apologies can no longer credit original source as lost to me)

Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.