
You are reviewing the ECG of a 40 year old lady with a background of hypoxic brain injury following Influenza A H1N1 ARDS who has presented with a reduced GCS from her nursing home.
Interpretation:
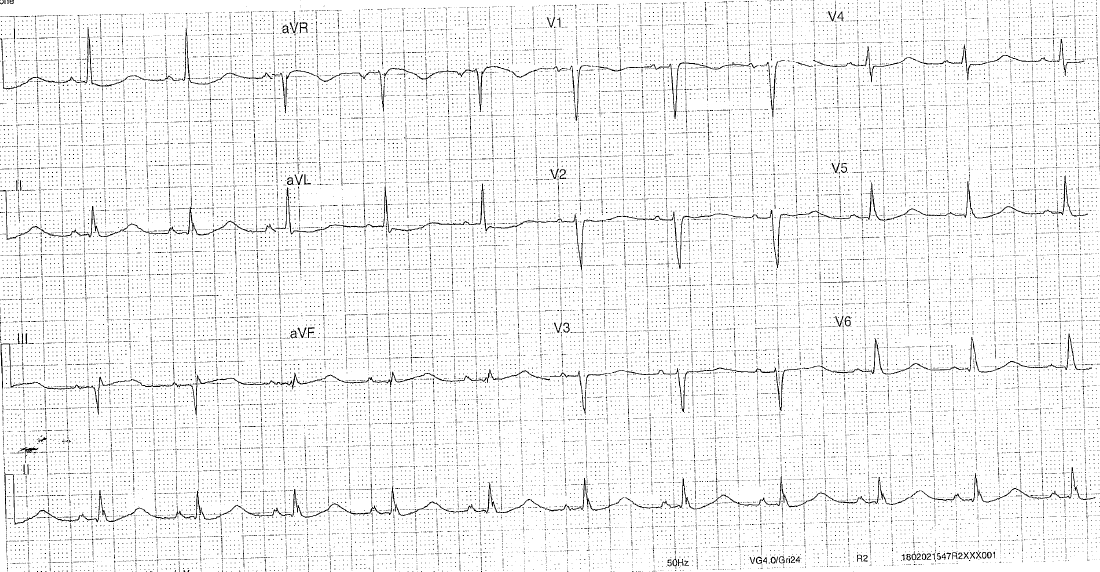
- Rate: 66
- Rhythm: sinus rhythm
- Axis: normal
- Morphology: high lateral and lateral STD, very flat T waves that appear dragged out (actually down up T and U fusion – seen best in lead I – pathognomonic for hypokalaemia)
- Intervals: PR 180 QRS 100 QTc 480 per machine interpretation, manual measurement Bazzett 610 – maximum slope technique (choose the biggest slopiest T wave) – this is an example of pseudo QT prolongation
- Summary: Hypokalaemia
Clinical closure:
K was 1.8 (and despite 60mmol of KCL replacement increased to only 2,5)
Mg 0.67
(rest of renal function Na 140, Cl 83, HCO3 40, cCa 2.82 – so the metabolic alkalosis in this patient could be the driving cause of her hypokalaemia)
The cause of hypokalaemia in this patient was not fully investigated further as the decision was made for antibiotics and fluids as a ceiling of care given the patients co-morbidities and pre-morbid status. She had ongoing high fevers and signs of sepsis 2 days after admission, and ultimately her treating team chose for comfort measures and treatment after she failed to respond.
Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
Further online reading:
Big thanks to Dr John Larkin as usual.
Please read his post on hypokalaemia here: