
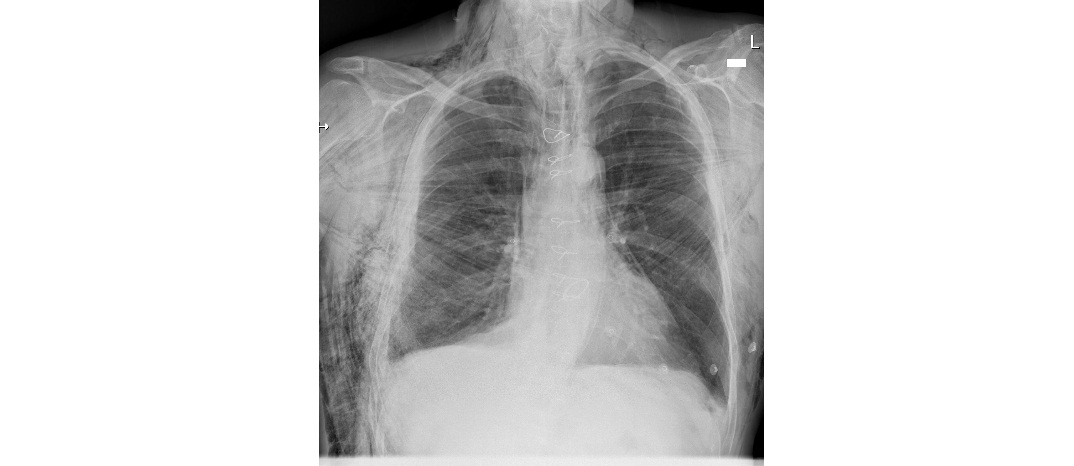
It is 1 am and you have just seen a 70 year old man in resus who has had a fall earlier in the night from a ladder. He is complaining of right sided chest pain. You request a trauma series. The chest x-ray is as follows. What can you see?
Click to enlarge
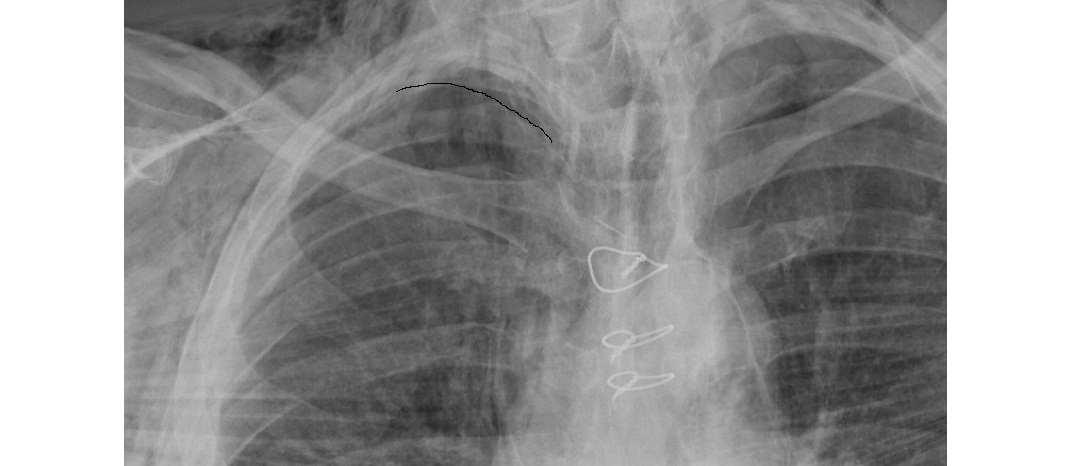
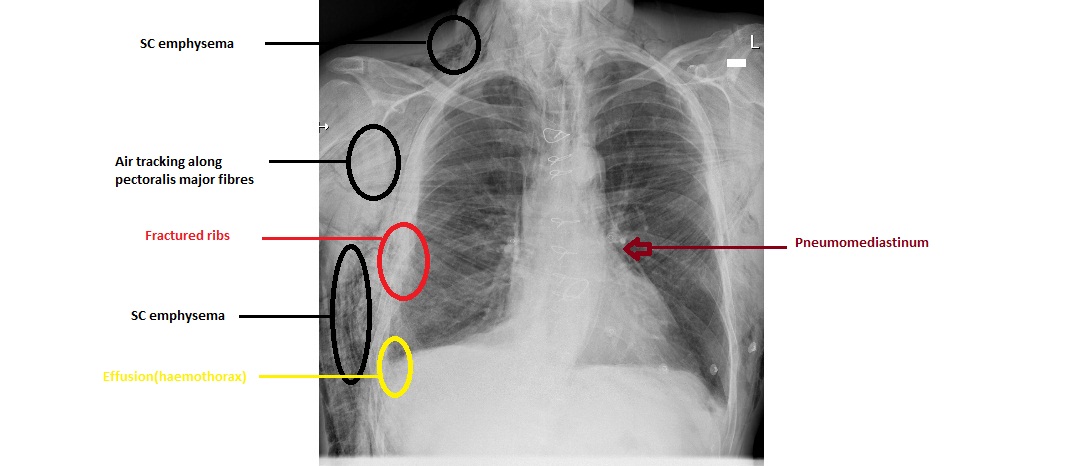
The chest x-ray looks alarming. There is an extensive subcutaneous emphysema involving the chest wall and the neck. There is pneumomediastinum. The patient also has a small right sided pleural effusion (haemothorax). There is a fracture of the middle ribs on the right (6-8th ribs on CT chest). There is a replaced aortic valve and there are sternotomy wires. On the close up view, you can see a small apical pneumothorax.

Click to enlarge
Click to enlarge
Click to enlarge
This patient has concerning injuries. Apart from his age and background emphysema history, he was also on warfarin for the metal aortic valve. He did not need a chest drain and was managed conservatively. The chest x-ray 6 days post initial presentation is as follows:

Click to enlarge
Subcutaneous emphysema can make interpretation of chest x-ray tricky. Detection of pneumothorax can be difficult on the chest x-ray as well as the bedside ultrasound. CT is the diagnostic test to characterise underlying injuries.
Apart from medical conditions and trauma related to airway structures and lung, another important not to be missed cause of subcutaneous emphysema is Boerhaave’s syndrome (distal oesophageal rupture secondary to vomiting etc). There are case reports of subcutaneous emphysema following sinus injury, dental procedures, pneumoperitoneum, laparoscopic procedures.
Air may track to the face, neck and deeper into the mediastinum. Although on its own, it is usually harmless, rarely it can cause upper airway obstruction and tension pneumomediastinum.
[/peekaboo_content]