
AXR – am I correctly positioned?
You are on a night shift and your next patient is a 40 year old woman who presents with vomiting and she also gives history of some runny stools. She has a lap band in situ and according to her, some fluid was taken out by her specialist about 12 hours ago and she had felt slightly better post deflation of the band. But she decided to present to ED as there was ongoing vomiting. She asks you if her symptoms could still be related to the band. Part of your mind thinks she is fine. She has just seen her specialist and has had fluid taken out. You also tend to think that she has `gastro` and nothing else. But because you do not want to miss anything, you decide to obtain an abdominal xray to check the band position.You are looking at the xray when the nursing staff comes to you wanting to know if the patient can be moved out of the gastro room. Here is the xray:

Would you send her home? What does the xray show?
[peekaboo_link name=”Answer”]Answer[/peekaboo_link]
[peekaboo_content name=”Answer”]
The AXR shows an incorrectly positioned/slipped gastric band with distension of the gastric fundus above.
A well-positioned band is at 30-45 degree angle from the horizontal at the gastroesophageal junction. Here is an example:


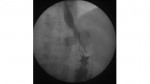
Here is a gastrograffin swallow showing a correctly positioned band:
A quick recap of lapband complications:
Early postop period – Gastro-oesophageal obstruction due to oedema or proximal migration of the band.
Chronic – migration/ slippage, overinflation of the band, gastric erosion (patient can develop intra abdominal sepsis), gastrocutaneous fistulas, port site infection, tubing disconnection from the port.
[/peekaboo_content]
This is great, Prathiba! Other chronic complication worth mentioning is that they are all high Anaesthetic risk, as the pouch above the band will always have food residue in it, that they passively “regurgitate” and sometimes aspirate.
Thanks Ioana.
Hi Prathibha,
Thanks for covering lap band slippage, an increasingly common presentation to the ED.
Nice article on the “O Sign” in lap band slippage, link below.
http://www.ajronline.org/content/195/1/137.full.pdf+html?sid=3a378c55-eb66-4829-96f3-6b9d3ef531d5
Thanks,
John
Thank you so much John.Nice article.Definitely worth reading.