A 60 year old diabetic patient with confusion and vomiting.
His VBG shows
Metabolic Acidosis –ph6.89 and HCO3- 6
Compensation – Expected CO2= (1.5×6 )+8 =17. CO2 of 32, therefore not fully compensated or underlying respiratory acidosis
AG = 109 –(72 +6)=31 Raised
Delta Gap =(AG-12)/(24-HCO3) =1 Therefore HAGMA
Osmolality = (2×102) +43+83=330
Corrected Na = Na + (glucose-5)/3 = 135
Potassium 7.6, Cr 1400 Glucose 83, lactate 6, HB 102
Description – HAGMA, with underlying respiratory acidosis. Severely high potassium. Marked hyperglycaemia with a hyperosmolality. Also noted is a marked raised urea and creatinine
Interpretation – In the clinical context the gas would be consistant with renal failure and a lactic acidosis causing HAGMA. The cause of the renal failure could be secondary to dehydration from vomiting, however renal and post renal causes should be excluded. The lactic acidosis is likely a combination of shock as well as the use of metformin. The patient has a critically high potatssium, which could account for the bradycardia, and urgent ECG and lowering of potassium is required. The patient has a markedly elevated glucose and a high osmolality, which would indicate HHS.
The altered mental state could be causing hypoventilation and the associated respiratory acidosis, but an underlying pneumonia needs to be excluded.
Management
Resuscitation- Treatment for the hyperkalaemia – calcium chloride, sodium bircabonate, salbutomol nebs, insulin and dextrose in acute setting
-management of bradycardia and hypotension –treatment of potassium might increase HR and ultimately BP, but fluid boluses required. If not responding inotropic support
-warm patient –bear hugger, warm fluids
-intubation if GCS does not improve with increasing BP and warming patient. Need to optimise patient prior to intubation and consider drug choices for induction that will not further decrease BP and increase potassium. Also will need to continue to bag the patient during induction and give NaHCO3, inorder not to worsen the acidosis (this patients GCS markedly improved with warming and increasing BP)
-continuous cardiac monitoring, urinary catheter, invasive BP measurement
Specific Management
-dialysis
-actively seek and treat underlying cause for renal failure and HHS
-antibiotics for underlying sepsis
-management of HHS
-avoid and withdraw nephrotoxic drugs
Disposition
ICU
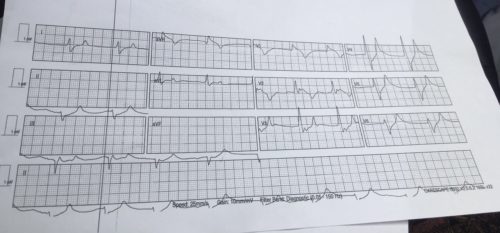
ECG for case