
Question 1
PH = 7.47 that is mild alkalaemia.
HCO3 = 39.2 accordingly we have metabolic alkalosis
Next compensation: expected PCO2 = 0.7 x HCO3 + 20 (range: +/- 5).
0.7 x 39.2 + 20 = 47.4 (Range 42.7 to 52.7).
PCO2 is 57, that is higher than the expected PCO2 so we have additional respiratory acidosis.
K = 2.2 that is moderate hypokalaemia
Cl = 89 that is hypochloremia.
Lactate = 1.2 mmol/L (Normal lactate level in unstressed patients is 0.5-1 mmol/L. Patients with critical illness can be considered to have normal lactate concentrations of less than 2 mmol/L.).
This interpretation will change slightly as that was venous blood (Not arterial). Major differences in levels between arterial and venous blood.
pH ABG vs. VBG: VBG pH 0.03–0.05 lower
HCO3 ABG vs. VBG: VBG HCO3 1.5–2.0 lower
CO2 ABG vs. VBG: VBG CO2 6-8 mmHg higher
O2 ABG vs. VBG: O2 VBG is not reliable.
And accordingly we can consider PCO2 within expected compensation range.
Question 2:
We use the mnemonic of CLEVER PD for the differential diagnosis of Metabolic Alkalosis.
C – contraction (dehydration)
L – liquorice (diuretic), laxative abuse
E – endocrine (Conn’s, Cushing’s)
V – vomiting, GI loss (villous adenoma)
E – excess alkali (antacids)
R – renal (Bartter’s), severe K depletion
P – post hypercapnia
D – diuretics.
The body loses K in three potential ways:
GI loss
Urinary loss
Intracellular shifting.
Hypokalaemic, Hypochloraemic metabolic alkalosis is the classical description of pyloric stenosis blood gas… Can this patient have Pyloric stenosis???
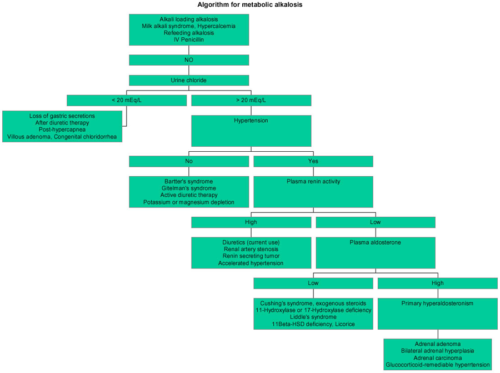
Metabolic alkalosis diagnostic flow chart
Question 3:
Treatment is by replacing K,
Consider replacing Mg
Magnesium deficiency is frequently associated with hypokalemia. Concomitant magnesium deficiency aggravates hypokalemia and renders it refractory to treatment by potassium.
Indications of admission in patient with Bulimia/ feeding disorder:
• Severe malnutrition (weight < 75% of average for sex, age and height)
• Dehydration & electrolytes abnormalities (K, Mg and PHO3).
• Physiological instability (HR< 50, Bl/Pr < 80/50 or postural drop, Temp < 35.6)
• Arrested growth or development.
• Failure of outpatient treatment or acute food refusal
• Uncontrollable binging and purging
• Acute psychiatric emergency (Suicidal or psychotic)
• Acute medical complication of malnutrition (syncope, seizure, arrhythmia or pancreatitis).
• Comorbid diagnosis that interferes with treatment (severe depression, OCD, severe family dysfunction).