
A 52 year old male presents to ED with shortness of breath for the last 2 weeks. The patient had been on a 6 hour flight 2 weeks ago.
Describe and Interpret the ECG
Answer:
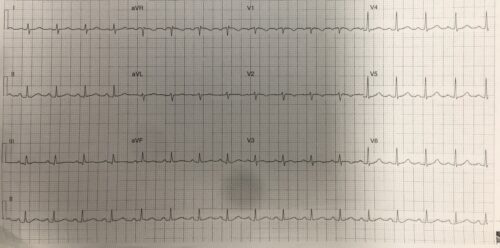
Rate: 102 beats/min
Rhythm: Sinus tachycardia
Axis: Normal axis
Intervals:
PR: 160ms
QRS: 90ms
QTc: 430ms
Additional:
TWI inversion V2
Flattened T waves III and aVF
S wave I
The above ECG shows a sinus tachycardia with some T wave changes in the inferior and anterior leads. In the clinical context of a recent flight and SOB, a PE needs to be excluded
Changes on ECG due to pulmonary emboli include
- Normal ECG (18%)
- Sinus tachycardia (44%)
- Anterior T wave inveriosn (34%)
- RBBB (18%)
- S1Q3T3 (20%)
- P Pulmonale (9%)
- Right Axis Deviation (16%)
- Atrial Fib/Flutter (8%)
This patient had extensive PE’s involving the lobar pulmonary arteries with a troponin rise of >1000 and right heart strain on CT and echo.
There are numerous findings on ECG in patients with PE’s. The ECG can neither diagnose or exclude the diagnosis of PE
References:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.