
The ECG below is taken from an 84 year old Nursing Home resident who complained of chest pain after a seated syncope. On examination his observations are within normal limits and he has mechanical heart sounds.
Interpretation:
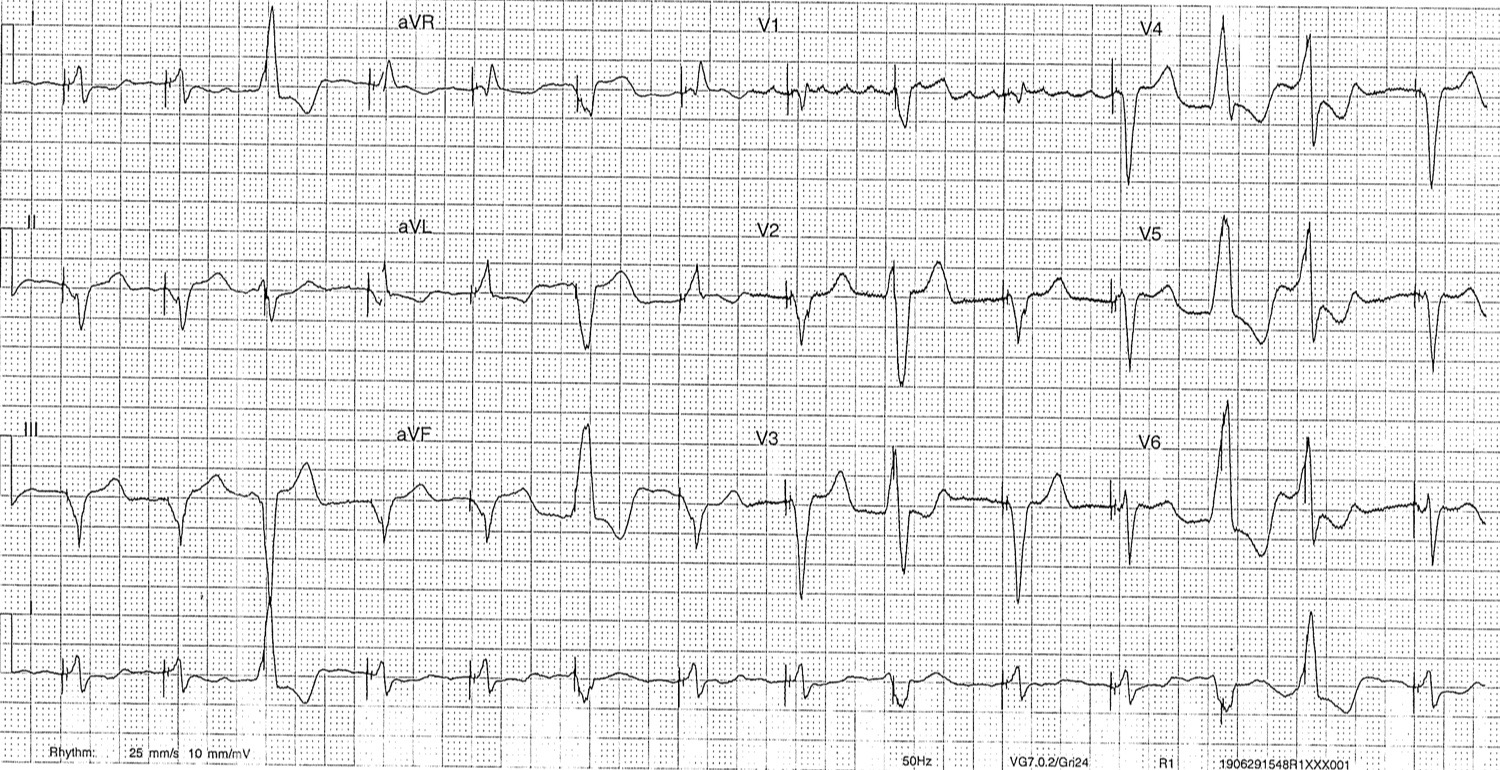
- Rate: 84
- Rhythm: Ventricular pacing with ventricular ectopics
- Axis: LAD
- Morphology: As consistent with pacing (QRS of LBB morphology, QRS and T waves discordant, poor R wave progression V1-6)
- Pacing: spikes seen in ectopic complexes but given they are ectopics unable to comment on whether this is a failure to sense vs appropriate pacing (ie did the ectopic impulse reach the pacing lead before or after the pacing spike – we can’t be sure)
- Scargbossa Criteria: not met
- Summary: Paced rhythm, possible failure to sense (can’t be certain)
Diagnosis:
- Cardiac dysrhythmia
- NSTEMI
- PE (unlikely given warfarinised for MVR and compliant, INR was appropriate)
Management:
Investigations:
- Serial ECGs (no change)
- CXR: metallic MV, moderately enlarged heart, no alternative cause for pain found
- Bloods: mild renal failure, Trop 117 -> 123 -> 92
- Previous Echo LEVF 15%
- PPM Interrogation: no problems.
Treatment:
- Ensure pain free: GTN as BP allows +- Morphine
- a discussion point here is whether to use GTN given Infr MI can be a cause of failure to sense but this patient was already pain free
- Anticoagulate: already taking aspirin, already on warfarin for MVR, decision made not for further antiPLT given age and risk of falls vs risk of benefit.
- Angiogram: again decision made not to angio given renal function and age / pre-morbid function (medical management chosen)
- Review by Cardiology – diagnosis of NSTEMI felt most likely.
Discussion Points:
Scargbossa in Paced Rythms
- Discordant STE >= 5mm (in Paced rhythms this is the most statistically important criteria)
- Concordant STE >= 1mm
- Concordant STD >= 1mm in V1/V2/V3
Pacemaker Problems:
- Failure to Sense – magnet application, battery / lead problem, MI
- Failure to Pace – both failure to output (battery / lead problem / oversensing) and failure to capture (settings problem / MI / fibrosis / drugs / pH or K states)
Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
With thanks to Dr Andrew Walker for his recent PPM teaching, and as always Dr John Larkin for being the font of all knowledge.