
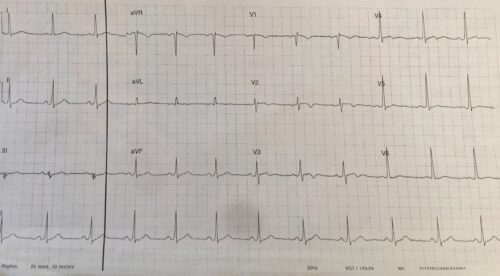
A 57 year old male presents o ED c/o pleuritic chest pain. The patient is otherwise well on no current medication. Below is his ECG:
Describe and Interpret the ECG
Answer:
Rate: 72 beats/min
Rhythm: Regular sinus rhythm
Axis: Normal Axis
Intervals:
PR: 160ms
QRS: 100ms
QTc: 438ms (Bazett)
Additional:
T wave inversion/Biphasic Twaves V2-4. Flattened T waves aVL
No Voltage criteria for LVH
ST elevation 1mm and dominant R wave V2
T wave inversion can be due to a number of pathologies including ACS, Wellens syndrome, BBB, LVH, Digitalis effect, CNS injury, acute myopericarditis, PE, Paced rhythms, preexcitation syndromes, persistent juvenile T wave patterns, metabolic causes.
The inverted T waves in ACS are usually narrow and symmetric. In Wellens syndrome they are symmetric and deep. In PE’s they are varying magnitude and seen in the precordial leads. In LVH there is ST depression with asymmetric, biphasic or inverted T waves. In acute myopercarditis T wave inversion is frequently small in size and symmetric morphology. In Persistent Juvenile T wave pattern, T wave inversion occurs in precordial leads and usually evolves to upright T waves in early to mid teens.
In this clinical situations ACS, PE and myopericarditis needs to be excluded, given the character of the pain and age of the patient
References
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.