
A 78 year old male presents to ED complaining of chest pain. He has a PPM and ICD in situ. Below are 2 ECG’s of the patient while he is in ED.
Describe and Interpret the ECG’s
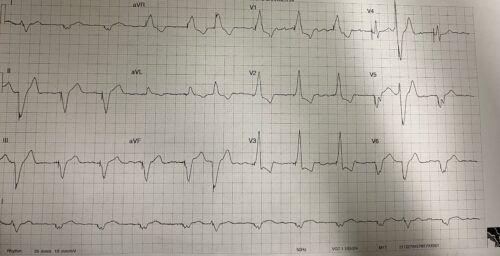
Rate: 72 beats/min
Rhythm: ventricular paced
Axis: Extreme Axis
Intervals
- PR – N/A
- QRS 184ms
- QT 526ms (Based on Bazett formula)
Additional:
- Ectopic beats 1,6 and 11 – pacing spikes within the ectopics
- RBBB morphology – LV paced
- QTc of 526ms is likely longer than actual QT in a paced rhythm – rough rule of thumb subtract 50ms from calculated QTc
ECG 1 shows a left ventricular paced rhythm, with PVC’s with undersensing. The QTc is on the upper end of normal even accounting for the paced rhythm
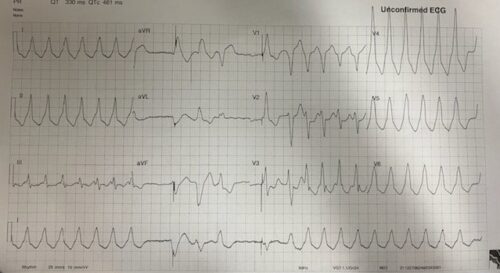
ECG2
1st quarter of ECG shows a unpaced wide complex tachycardia with a rate of around 150 beats per minute which self terminates after around 3 seconds
2nd quarter of ECG shows 3 wide complex PVC’s, with a pacing spike inappropriately placed in the first complex
2nd half of the ECG shows initial appropriately paced complex, followed by a complex that occurs before termination of the Twave of this complex. This is then followed by a sustained wide complex tachycardia at a rate of 150 beats per minute.
At no point does is there any sign of the ICD functioning during the VT
The above ECGs shows PVC’s with undersensing as well as runs of VT with no ICD function. The VT might be induced by R on T phenomenon due to ectopics. The ectopics might be a results of electrolyte disturbances, lead displacement, medication or ACS related.
References:
Chan et al, ECG in Emergency Medicine and Acute Care
Tang,J et al, Assessment of QT interval in ventricular paced rhythm: Derivation of a novel formula. Journal of Electrophysiology Vol 57 Pg 55-62