
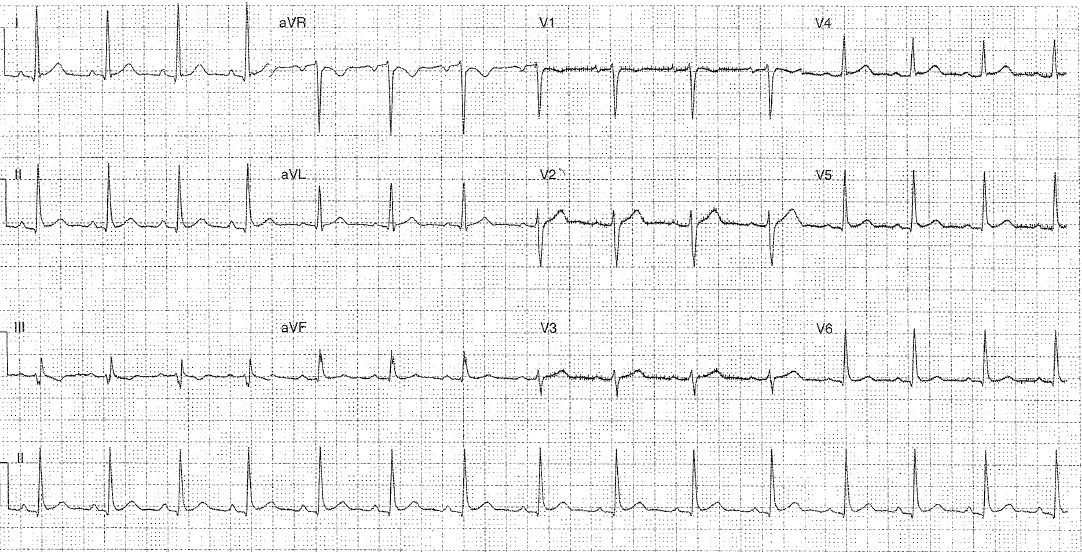
You see a 26 year old man who has presented with left sided chest pain. He self discharged 3 weeks ago from the cardiology ward. His ECG is as below.
Interpretation:
- Rhythm: sinus
- Rate: 90
- Axis: Normal (0-90)
- Morphology: PR depression (best seen lead II), upsloping p in aVR (knuckle sign), inferior Q waves, QRS fragmentation in III and aVF, possible spodick sign – TP downsloping best seen in leads V2/3, STE <1mm V5/6, meets voltage criteria for LVH (>15mm R and S wave in I and aVR.
- Intervals: PR170 QRS100 QTc390
- Summary: ?pericarditis/myopericarditis ddx in context of IV drug use or cardiac risk factors NSTEMI.
Spodick sign: the downsloping of the TP segment seen in 80% of pericarditis patients (Chaubey VK et al. 2014) Also can be positive in STEMI in 5% of patients (Whitting 2020)
Clinical closure: this man was known to have myopericarditis since 2018 thought secondary to THC use (1g / day). He presented with a pulse of 110 and a BP OF 120/82. He was afebrile with a RR of 16 and Sats of 98%. Clinical findings were muffled HS and a raised JVP. His bedside echo in ED showed a small effusion without tamponade. His cardiac MRI from January showed no scarring or infiltrates. Trop was 2, CRP 148 and WCC 14.5. During admission he suffered from THC withdrawal which was treated with diazepam. His formal Echo showed an EF of 56%. He was discharged on colchicine and a weaning dose of prednislone after a 4 day admission under the cardiology team.
Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.
References:
- Chaubey VK et al. Spodick’s Sign: A Helpful Electrocardiographic Clue to the Diagnosis of Acute Pericarditis. Perm J. 2014 Winter; 18(1): e122. doi: 10.7812/TPP/14-001
- Witting MD et al. Evaluation of Spodick’s Sign and Other Electrocardiographic Findings as Indicators of STEMI and Pericarditis. J Emerg Med. 2020 Mar 25. pii: S0736-4679(20)30020-2.