
86 year old male with a background of CRF, PPM and AF presents to ED with SOB
Answer
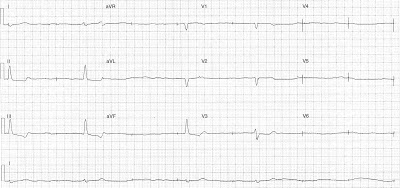
Rate: Ventricular rate 24 bpm
Rhythm: No P waves, irregular, AF
Axis: Normal
Intervals
- PR N/A
- QRS 120 ms
- QTc 405 ms
Additional:
Irregular pacing spikes at 42 bpm
ST depression inferiorly
The above ECG shows slow atrial fibrillation with pacemaker dysfunction. The down slopping ST depression and shortened QTc inferiorly maybe due to the digoxin effect.
Pacemaker dysfunction can be due to a number of causes:
- Failure to capture
- Failure to pace
- Undersensing
- Pacemaker mediated tachycardia
The above ECG is an example of failure to capture – pacing spikes are not followed by depolarisation. Causes of failure to capture include
- Device malfunction – pacing voltage programmed too low, lead dislodgement, lead fracture, low battery life, elevated pacing thresholds
- Patient issue – acute MI, electrolyte abnormalities (eg hyper K), metabolic derangement.
Further reading : Chan et al, ECG in Emergency Medicine