
It is 2 am again and you are about to see your next patient, a little old lady with abdominal pain and tachycardia.
You want to take a detailed and thorough history from her in regards to her abdominal pain but she couldn’t care less. She is conscious but prefers to keep her eyes shut and is wincing. You initially think that she is a ‘poor historian’ but finally figure out 10 minutes later that she is in a lot of pain. You manage to give her IV opioids and then examine her tummy. You plan to request an erect chest and abdominal x-ray as your 1st investigation. Her erect chest x-ray is here. On re-examination, she is getting more sick. What would you do next?
Air where it should not be!
Your next step should be to phone the on call surgical registrar and if not available, the surgical specialist as this is a surgical emergency. Erect chest xray shows a thin silver of air under the right diaphragm secondary to a perforated viscus. The abdominal x-rays essentially were normal (not attached here).
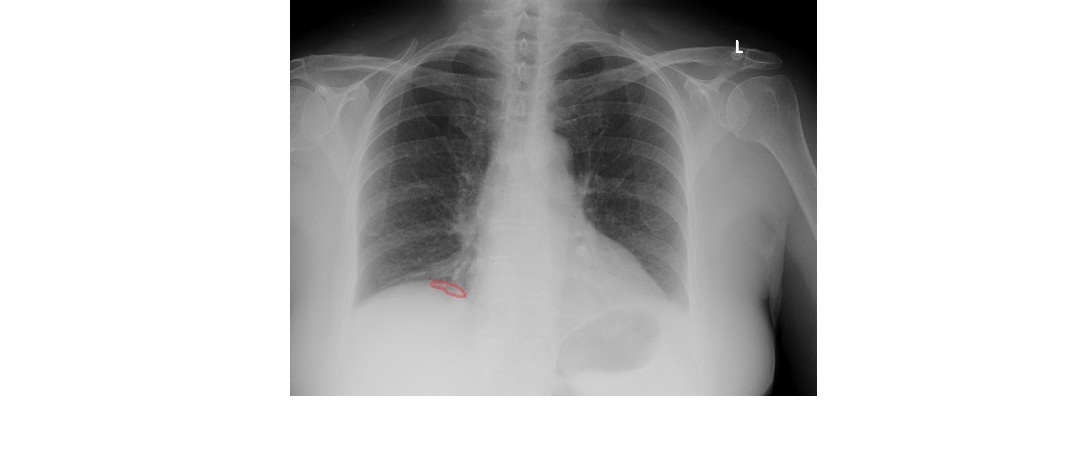
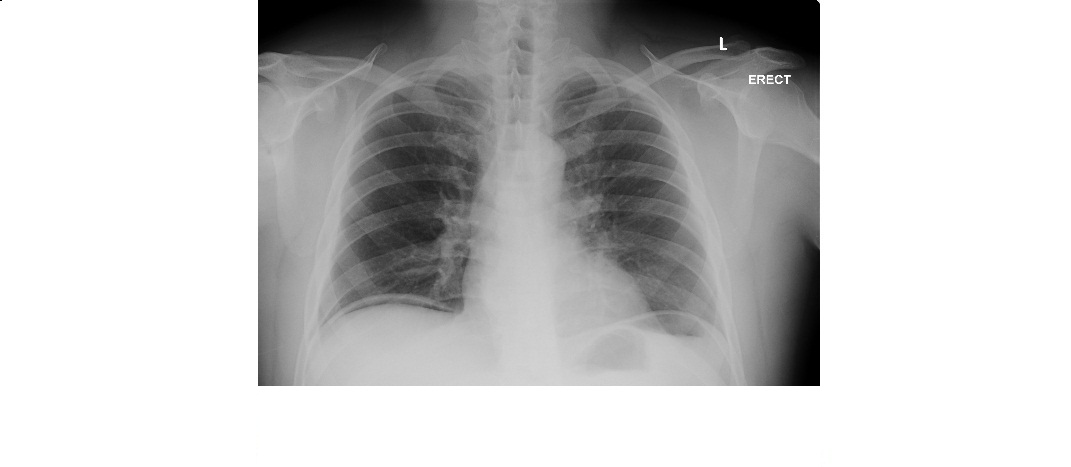
My intention to choose the above x-ray is to show how subtle the finding can be in pneumoperitoneum. You may not see large amount of air all the time as in the x-ray shown below.
Erect chest x-ray is only 80% sensitive to detect gas under the diaphragm. The sensitivity of an erect lateral chest x-ray is higher.
For erect chest x-ray, patients need to stand upright for at least 10 minutes. In sick patients, who are too unwell to stand, you can obtain a decubitus film to make a diagnosis. Left lateral decubitus film can show air against the hepatic shadow. But you should allow sufficient time for the air to rise (15-20 minutes). Not right lateral decubitus film as the fundal gas interferes with interpretation.
There are various other interesting signs mentioned in pneumoperitoneum – Rigler’s sign (both bowel walls well outlined by free intraperitoneal air), falciform ligament or Silver’s sign, football sign which is seen on supine radiographs as large oval translucent area (like an american football as per an article in RSNA!), continuous diaphragm sign etc.
As for your patient, she was operated on for a perforated duodenal ulcer and recovered well.
[/peekaboo_content]