
37 y/o female presented with a history of fever. A routine ECG was performed as the patient had a rapid pulse.
Interpretation:
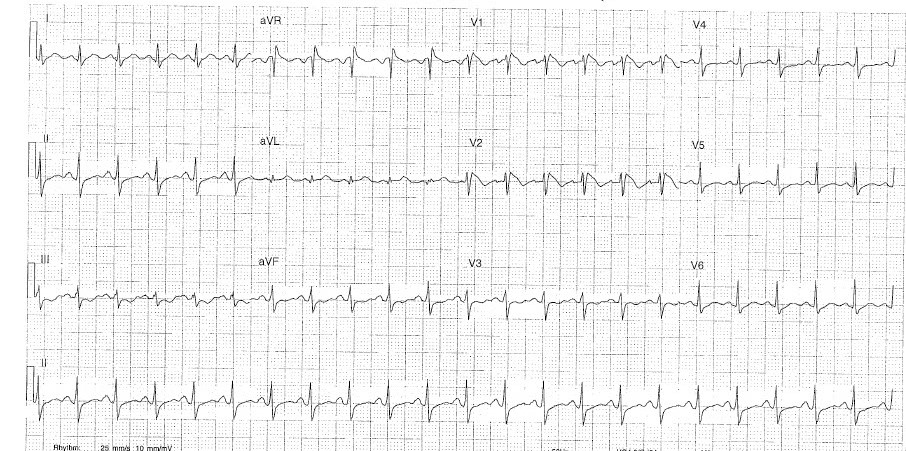
- Rate: 132 bpm
- Rhythm: Sinus
- Axis: Normal 0-90 degree
- Morphology: STE in V1
Coved ST-segment elevation >2mm in V2,
both STE followed by a negative T wave. (Brugada sign)
ST depression in lead 3 only ~ 1mm
- Intervals: PR – 120msec (normal)
QRS 92msec (normal)
QT interval corrected ~ 400 (Hodge’s formula)
- Summary: Type 1 Burgada Syndrome
(Brugada sign only ECG, This is the only ECG abnormality that is potentially diagnostic)
Brugada Syndrome Key Points
- There’s really only one type of Brugada syndrome.
- Diagnosis depends on a characteristic ECG finding ANDclinical criteria.
- Further risk stratification is controversial.
- Definitive treatment = ICD.
- Brugada sign in isolation is of questionable significance.
Brugada syndrome is due to a mutation in the cardiac sodium channel gene. This is often referred to as sodium channelopathy.
ECG changes can be transient with Brugada syndrome and can also be unmasked or augmented by multiple factors:
- Fever
- Ischaemia
- Multiple Drugs
- Sodium channel blockers eg: Flecainide, Propafenone
- Calcium channel blockers
- Alpha agonists
- Beta-Blockers
- Nitrates
- Cholinergic stimulation
- Cocaine
- Alcohol
- Hypokalaemia
- Hypothermia
- Post DC cardioversion
Type 1
- Coved ST-segment elevation >2mm in >1 of V1-V3 followed by a negative T wave.
- This is the only ECG abnormality that is potentially
- It is often referred to as the Brugada sign.
Management
The only proven therapy is an implantable cardioverter-defibrillator (ICD). Quinidine has been proposed as an alternative in settings where ICD’s are unavailable or where they would be inappropriate (eg: neonates).
Undiagnosed, Brugada syndrome has been estimated to have a mortality of 10% per year. Does this mean that a diagnosis in ED mandates admission? Probably yes for all type 1 patients if they present with suggestive clinical criteria.
It may be appropriate for risk stratification on an outpatient basis with an electrophysiology study (EPS) to see if the patient has inducible ventricular tachycardia (VT) or fibrillation (VF)in the following settings:
- Asymptomatic patients with a type 1 ECG pattern.
- All type 2 + 3 ECG patterns.
Ref: Life in the Fast lane
.
Fever in those with spontaneous Brugada Type 1 syndrome has been known to induce Type 1 EKG changes; it is recommended to aggressively treat any fever in these patients when identified. Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al. In a cohort of 588 patients with diagnosed Brugada syndrome who had an arrhythmic event, 6% were associated with a febrile illness. Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever
Ref: https://hqmeded-ecg.blogspot.com/search/label/brugada