
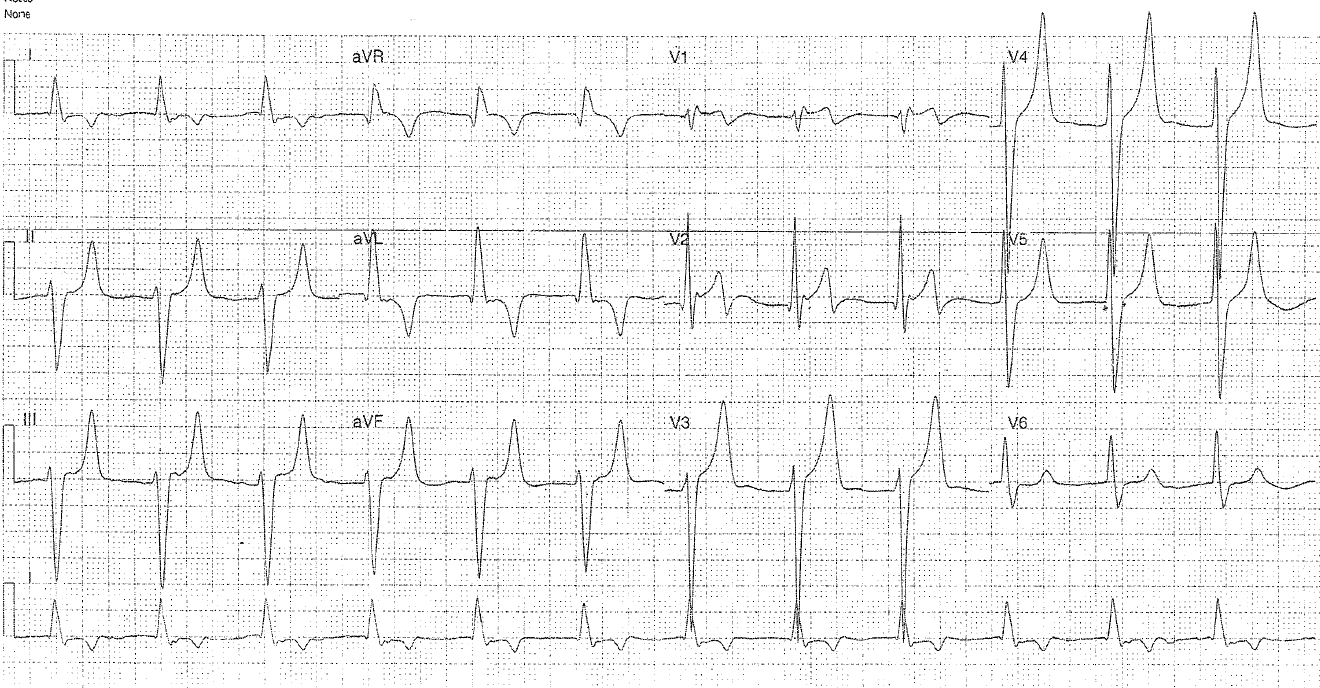
The ECG below is from a 66 year old diabetic man who has presented with sepsis.
Interpretation
- Rate: 72
- Rhythm: broad complex (likely inherent rhythm with p wave flattening)
- Axis: Extreme LAD
- Morphology: LVH criteria, peaked T waves (and ‘peaked’ inverted T was in aVL as seen with below diagnosis in LVH) flattened p waves best seen in V3 and V6, pseudo-brugada pattern in V1-2 (likely due to Na channel blockade effect seen in hypercalcaemia)
- Intervals: QRS >120, PR (seen best in V3 and V6) 400
- Summary: Hyperkalaemic ECG
Hyperkalaemia
- usually seen with K levels > 6.0
- Starts with increase in T wave amplitude as repolarisation is affected, followed by changes seen in atrial paralysis with p wave flattening or widening with eventual disappearance, and PR prolongation.
- Levels of >7 are associated with conduction disruption, with bundle branch and fascicular blocks as well as bradyarrhythmia and QRS widening.
- K>9 will be seen as the pre-terminal sine wave, followed by asysle, PEA with board complex patterns and VF.
Clinical Closure
K was 8.1
Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.