
It’s a surprisingly busy Sunday shift and you are reviewing a 72 year old lady with a background of hypertension who has presented with chest heaviness radiating into the arms, back and neck. She had experienced the back pain the day before and woke with new chest pain in the morning. On examination she looks pale and has a pacemaker scar but there is nil else to find.
Her ECG is as below:
 Interpretation:
Interpretation:
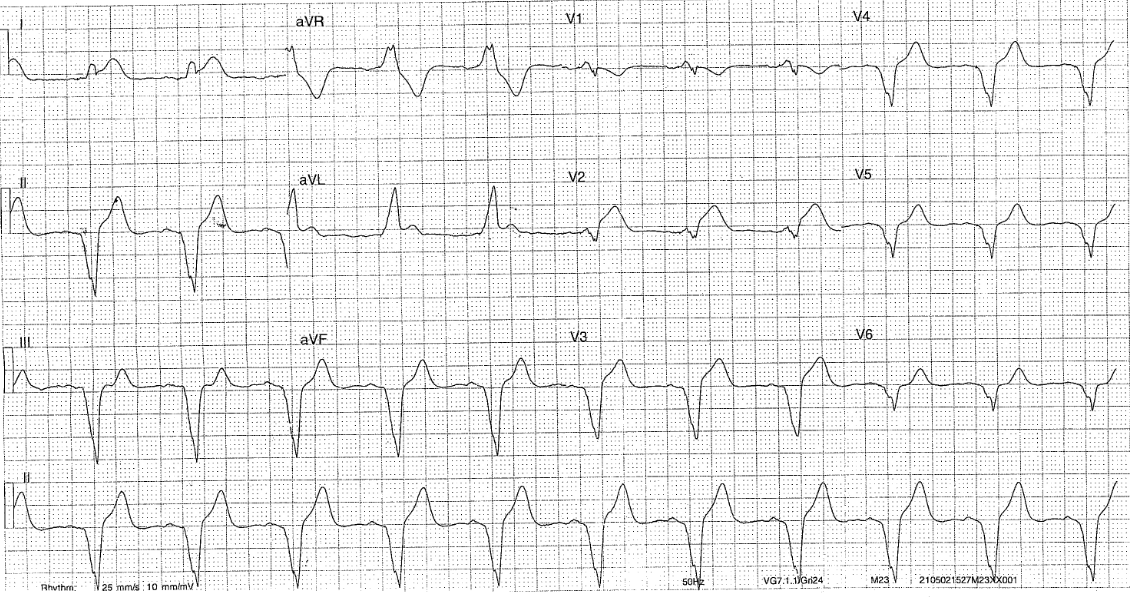
- Rate: 66
- Rhythm: paced ryhthm (spikes more easily seen in III and V2-V4)
- Axis: -30 to -90: LAD
- Morphology: concordant STE 1mm lead I and aVL, excessively discordant STE V2 >25% of preceeding s wave (Smith modified criteria) and approx 1mm STD V1
- Intervals: wide QRS consistent with pacing
- Summary: Scargbossa +ve chest pain, with a good story suspect STEMI equivalent ACS.
Management: as for STEMI: ie aspirin 300mg, GTN +- morphine or fentanyl to acheive pain score of 0/10, and this lady was also given Clopidogrel (as HR dropped to <50) and heparin bolus given her convincing story and exam (she was pale and sweaty and looked like she was having an MI)
In JHC out of hours STEMI equivalent cases are discussed with the cardiology consultant to decide whether these patients require urgent transfer to our local tertiary hospital SCGH for out of hours PCI.
Clinical Closure:
This patient had an increasing trop rise (at 4 hrs = 16, 6hrs = 903, 20hrs = 28876)
Ct aortogram showed no dissection
CT coronary angiogram showed a 99% stenosis of LAD which was stented.
Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.