
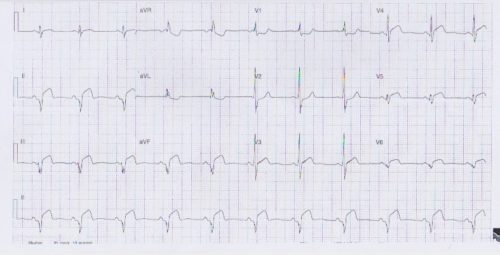
Following is an ECG of a 25 years old man with a four day history of left sided chest pain and its 0400 hours in the morning. He’s in a mild discomfort but looks well from the end of the bed and his observation were within normal limits. Describe the abnormalities, differential diagnosis and outline a management plan.
Interpretation:
- Rate: 66
- Rhythm: Sinus rhythm
- Axis: LAD
- Morphology:
- 3mm STE Infr leads
- 2mm convex STE Septolateral leads
- STD V1
- Pathological Q wave inferior leads
- >1mm wide >2mm deep >25% height QRS
- PR elevated aVR
- Intervals: Normal PR and QRS with RBBB pattern
- Summary: ?STEMI – Inferior septolateral ?myo-pericarditis ?coronary vasospasm (given age explore illicit drug use) ?-ve delta wave of WPW (given looks well and obs stable)
Clinical Closure:
- Admitted to cardiology at JHC
- Treated with aspirin / ticagrelor / heparin / analgesia
- CXR normal
- Trop 32000
- Angiogram – normal coronaries with mild focal inferior hypokinesis
- Echo – normal LV, akinesis mid inferior lateral walls, impaired systolic function EF51%, thickened infr-lateral wall (?oedema from myopericarditis), small circumferential pericardial effusion
- Rx of aspirin, Ramipril, metoprolol, ibuprofen
- F/u Echo in 2/12 – resolution of oedema, EF 57%