
You see a 77 year old diabetic lady with a one month history of SOBOE on a background of Rheumatic fever as a child. On examination she has a pan systolic murmur.
Discussion:
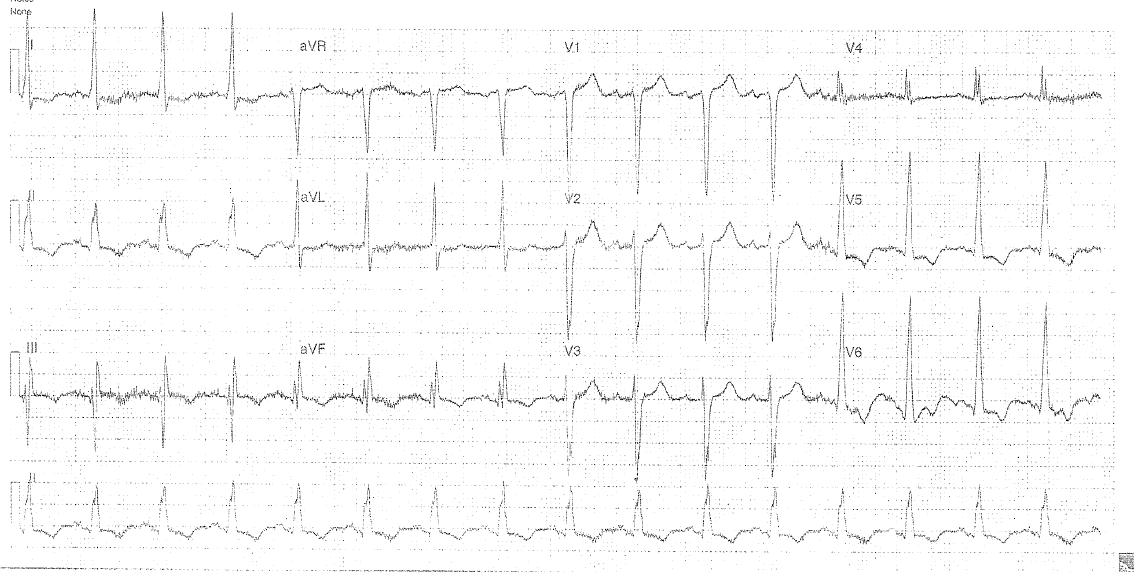
- Rate: 90
- Rhythm: NSR
- Axis: LAD
- Morphology:
- increased amplitude QRS +
- strain pattern
- (fitting both voltage and non-voltage criteria for LVH)
- for further reading see LITFL link below
- LAA (LA abnormality)
- p wave>0.12 sec
- often biphasic – esp V1
- or bifid (p mitrale) – esp in limb leads
- Intervals: PR150 QRS120
- Summary: LVH with features consistent with Mitral Regurg (see below)
Features Seen in Mitral Regurgitation:
- LA abnormality as discussed above
- almost always assoc with LVH
- Cf features in Mitral Stenosis of LAA +- RVH + often assoc with AF.
Clinical Closure:
This lady was in clinical APO, and was treated with IV diuresis and fluid restriction. Angio showed extensive coronary artery disease, the circumflex being the only vessel without complete occlusion (medically managed therefore but prognosis extremely poor) Echo showed an extremely dilated LV which was diffusely hypokinetic. EF was 15%. LA was mildly dilated, MR was moderate. There was also evidence of an old infr MI. She was discharged home after an 11 day stay.
Further Reading – Online:
You can read about the voltage and non-voltage criteria of LVH at Life in the Fast Lane via the link below:
Further Reading – Textbook:
Chan TC, Brady WJ, Harrigan RA, Ornato JP, Rosen P. ECG in Emergency Medicine and Acute Care. Elsevier Mosby 2005.