
ECG of the Week 28th December 2022 – Interpretation
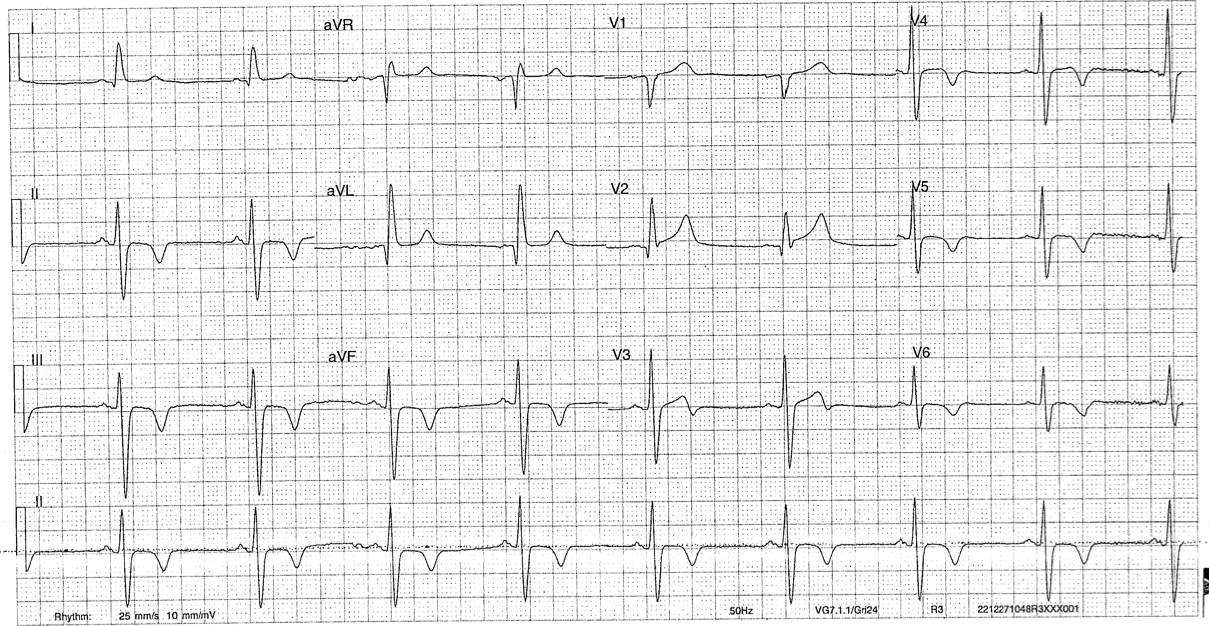
The patient is in a sinus rhythm with bradycardia (rate ~50) without evidence of AV nodal blockade. The QRS complexes are narrow. The most marked abnormality is widespread T wave inversion inferolaterally (II, III, AVF, V3 – V6). The T waves are upright in aVR and V1, and almost appear hyper acute in V2. This is distinct from an ECG he had approximately 30 minutes ago. His pain responded well to dual antiplatelet loading, GTN and a heparin infusion. He remained haemodynamically stable despite some occasional runs of bigeminy.
His larger clinical picture and important priorities to qualify include:
- He has mentioned that he doesn’t want to be resuscitated on his own accord. This is a great opportunity to discuss goals of care with the patient and his family members. It needs to be clarified if (1) he suffers from any form of mental illness / thought disorder that would preclude him from making this decision – hypercalcaemia, brain metastasis, cerebritis from his myeloma therapy (2) this has been discussed with his family members – gives more evidence to a thought out and considered decision (3) what therapies he considers invasive and acceptable – is a coronary angiogram acceptable?
- Is there anything specific about Carfilzomib that we need to know (or any other newer therapies for that matter) – it is contributory to his ACS presentation? Are any antiplatelets or anticoagulants contraindicated?
- What is his prognosis from myeloma with the specific therapy he is receiving and are there ramifications for his next chemotherapy cycle? – it would be sensible to touch base with his private haematologist.