30 year old male presents to ED with complaint of right knee pain, swelling and difficult to put weight on it for last 24 hours. He generally feels unwell with it. No previous history of same and otherwise healthy. He sustained small abrasion to his knee after a fall at work about 1 week ago.
His vitals : HR 100, BP stable. temp 38.5 , RR 18.
Knee Exam: swollen knee, with erythema . PROM 0-40 degree, and can not walk because of the pain. He gets initial investigations and also undergoes knee aspiration in ED with following results.
Colour: yellow and opaque.
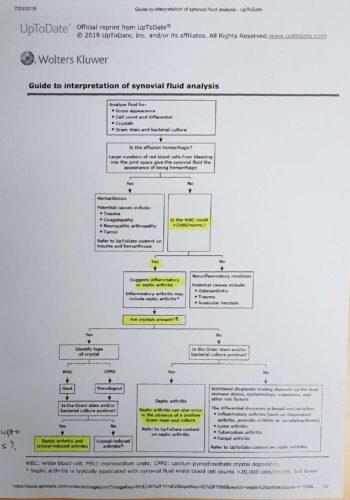
WBC : 25, 000 / ml
Polymorphs: 78 percent.
crystals ; negative.
Gram stain and cultures pending….
Questions:
- What is your differential diagnosis based on history and examination ?
- What investigations you will consider?
- How will you manage him based on above aspirate results. ?
Answers :
- Differential Diagnosis:
Septic arthritis, Crystal arthropathies ( gout / pseudo gout), Cellulitis, prepatellar bursitis. Others include viral or fungal arthritis, acute traumatic arthritis.
2. Investigations:
Bloods : FBC, UE, CRP , Blood Cultures. > Raised inflammatory markers strongly suggest inflammatory / infectious arthritis. CRP rises within few hors of infection and trend of reading helps regarding efficacy of treatment.
Knee Xray : Helps to determine if concurrent bony or joint problem. Also identifies joint effusion. USG can confirm joint effusion and helps with aspirate. MRI of joint can help identifying joint effusion and associated bony abnormalities e.g osteomyelitis especially in kids.
Knee aspiration : Gold standard for diagnosis and directed antibiotic treatment/ washout.
Send sample for Cell count, crystals, cultures, and gram stain.
Lactate, glucose levels, and LDH are useful to add if patient is already on antibiotics treatment , hence reduced glucose levels point toward infective cause.
Remember: Gram stains are positive in only 1/3 of cases. 5 percent of patients with crystal arthropathies will also have septic arthritis.
- Management : above aspirate results and clinical picture are very concerning for septic arthritis. Adequate analgesia, Nil by mouth and urgent discussion with orthopedic team should be sought. With hold any IV antibiotics and discuss with orthopedic colleagues as usually they prefer giving antibiotics during joint wash out .
Interpretation of aspirate : WBC > 50,000 strongly suggestive of septic arthritis. Cell count > 20,000 with polymorphs > 75 percent also suggestive of septic arthritis. Upto 5 percent of patients can have crystal arthopathy and septic arthritis.
In ED we should have low threshold to consult orthopedic team with any WBC > 20,000 and final decision / plan should be based on whole clinical picture