
23 years old female presents to emergency department with c/o neck pain and upper thoracic cage pain for last 2 weeks. Patient has been taking regular analgesia with temporary relief. No significant past medical history. Otherwise well. No trauma.
HR 90, BP 117/80, afebrile, RR 18, sats 100 RA.
chest clear, abdomen soft non tender. Patient was discharged home after brief work up in ED and advised to follow up with GP. Patient was seen by GP few days later and bloods were requested. results are as followed:
Hb 110
WCC 12
Platelets 170
Bilirubin 18 ( < 21)
Alkaline phosphatase 450 ( 30-110)
GGT 50 ( < 51)
ALT 30 ( < 56)
Urea, electrolytes: normal.
Answers:
1. significantly raised alkaline phosphatase level.
2: In the presence of normal bilirubin and other liver enzyme levels , non hepatic causes of raised ALP should be considered. The main ones are as below.
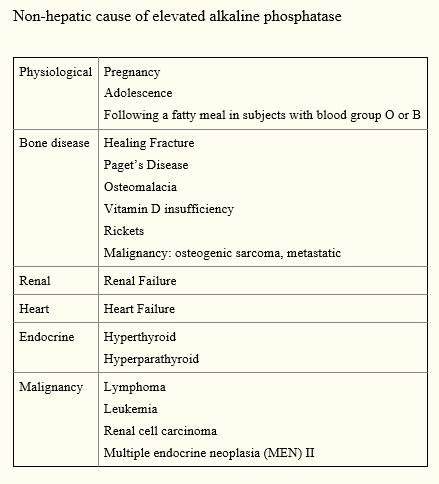
3: In the absence of any features of heart failure, renal failure, clinical hyperthyroid state , musculoskeletal and malignant causes should be on top of the list. It is appropriate to start with plain C spine and CXR films to find any obvious lesions in this patient.
Patient infact had a CT c spine from GP which showed multiple lytic lesions in c spine almost causing pathological fracture of upper cervicle vertebrae. Patient was referred back to emergency and had further imaging showing an ovarian mass ( malignant) which had metastasized into the spine and rib cage causing raised ALP levels.